4-channel Integration Engine
HL7 v2.5.1 MLLP (port 2575) · FHIR R4 REST · IHE PDQm/PIXm · CSV bulk import — all four live in v0.1.6.
✓ liveOpenMPI links the same patient across every system in your trust or your ICS — EPR, PAS, Lab, Radiology, ED, Maternity, MH, Community, Social Care — and across every assigning authority — NHS number, MRN, hospital number, MPI surrogate keys.
We use LLM + agent SDKs to reason about ambiguous candidate pairs alongside a Fellegi-Sunter probabilistic engine and a human steward console — with full DCB0129 / DCB0160 clinical-safety evidence on every release.
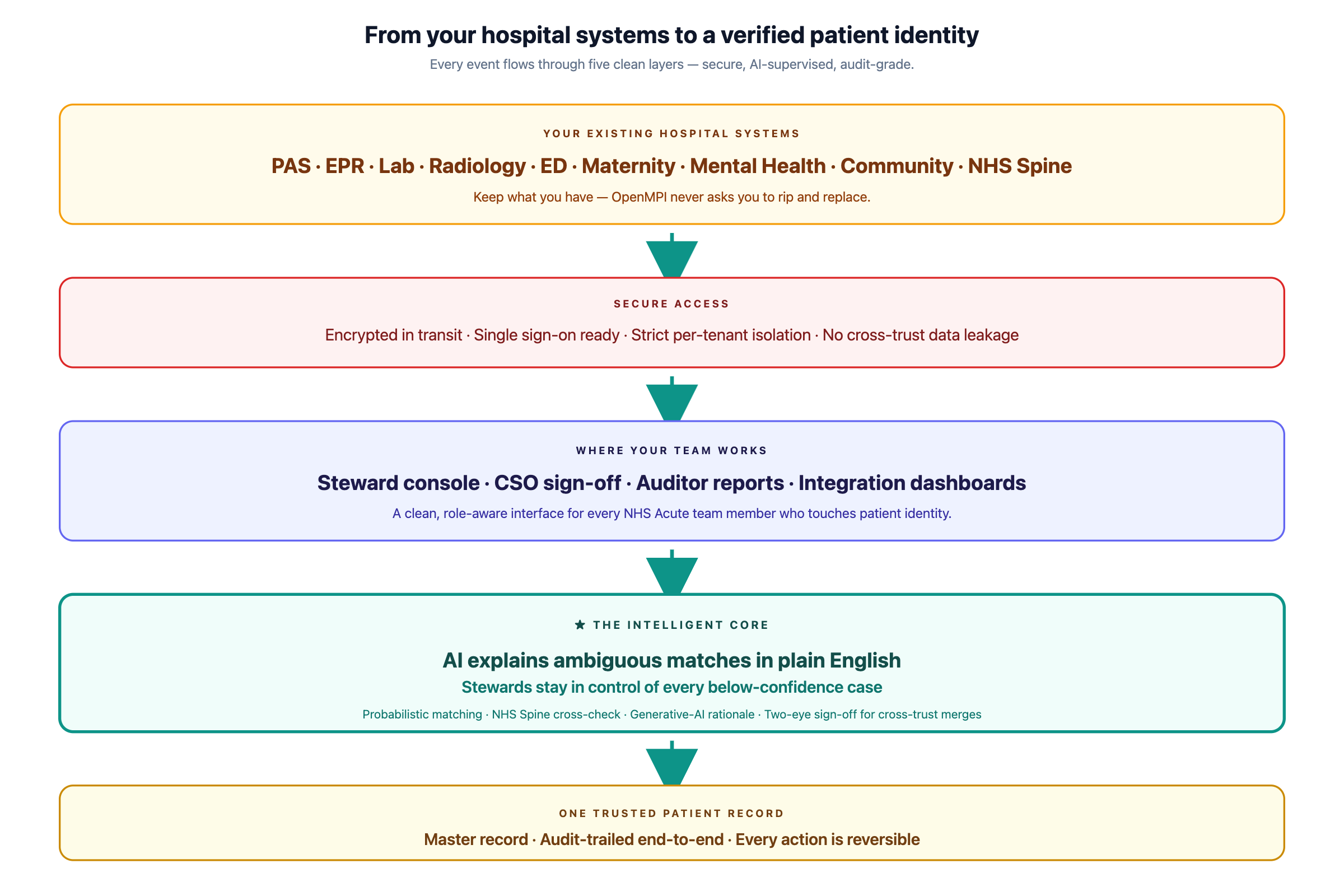
From your existing hospital systems, through secure access and an AI-supervised matching core, to one trusted patient record — audit-trailed end-to-end.
Traditional MPI platforms still rely on a human to manually dictate every borderline link — a slow, expensive, error-prone bottleneck that grows with the trust. OpenMPI closes that gap with machine intelligence that reads each ambiguous case, surfaces the relevant evidence in plain English, and routes the right question to the right person — driving steward productivity up by 2–4×. The AI never decides on its own. Your humans always make the call; the AI just makes sure they make it faster, with better information, and an audit trail behind every action.
| Pain in legacy MPI / EMPI | OpenMPI |
|---|---|
| Probabilistic algorithms need re-tuning per source system | Per-source-pair F-S calibration · CSO-co-signed threshold lifecycle · KDE-valley statistical proposer (v0.1.7) |
| Steward worklists drown in low-yield tasks | L5 LLM-Agent rationale prioritises high-yield work · 2–4× steward productivity |
| Match decisions are opaque ("score 0.83") | Per-feature breakdown plus AI rationale block on every below-T_AL decision |
| Cross-EPR merges in HIOW-style multi-trust ICSs are manual | Two-eye agentic cross-trust merge · CSO-grade evidence · SHA-512 audit chain |
| NHS Spine PDS sync is brittle | First-class PDS-FHIR client (v0.1.7) · Mod-11 validator live · discrepancy reasoning |
| Setup is months | Cloud-native SaaS · 4 deployment tiers · BYOK from tier 2 |
Everything that ships in v0.1.7 — backend code, frontend surface, audit + clinical-safety evidence.
HL7 v2.5.1 MLLP (port 2575) · FHIR R4 REST · IHE PDQm/PIXm · CSV bulk import — all four live in v0.1.6.
✓ liveL0 Validate → L6 Steward · literature-seeded Fellegi-Sunter · multi-row demographics blocking · per-source-pair calibration.
✓ liveConstrained tool-use over Haiku → Opus tiering · per-feature evidence + pre-vote · never alters the numeric score.
⚙ mock-only · real v0.4First-class NHS Spine PDS-FHIR client · NHS Modulus-11 validator live · NHS Data Dictionary codesystems seeded.
⚙ mock · real v0.1.74-band decision model · 3 configurable thresholds · Worklist · Candidate-Pair Review with side-by-side breakdown.
✓ liveStructural row-level scoping · 8-role × ~50-action × 5-level RBAC matrix · cross-tenant isolation regression.
✓ live18 hazards seeded · re-evaluated each release · CSO-signed CSCR · production-activation gate explicitly closed in v0.1.x.
✓ livePer-tenant pg_advisory_xact_lock · monthly partitioning · verify_chain() exposes ✓ intact / ⚠ broken.
✓ live4 protected groups (Anglo · South-Asian · East-Asian · Eastern-European) · ≥ T_RL on near-match · ≤ 10pt gap.
✓ liveUUID v4 internal-by-default · stable across mergers · splits · PAS replacements · NHS-no supersession · optional virtual OPENMPI_ID AA.
✓ liveSame engine for any entity_kind · patient is v1.0 primary · practitioner / organisation / device / specimen / episode structurally ready.
✓ architectured5 visual states · drill-down breakdown · per-tenant daily ceiling · runner real-token mode requires per-run authorisation.
✓ liveSeven clear steps from raw demographics to a confident outcome. The AI explains every borderline case in plain English — and your stewards always decide what happens below the auto-link line.
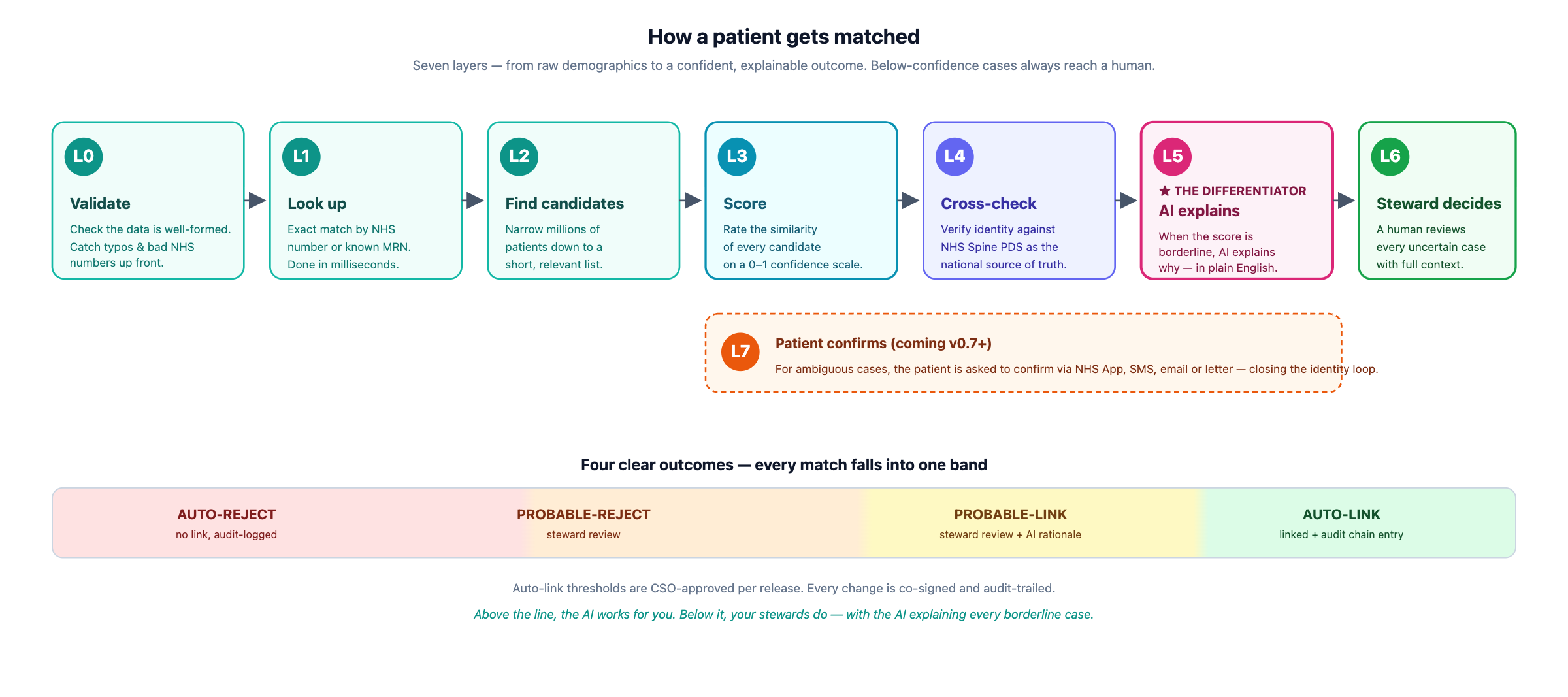
Auto-link thresholds are CSO-approved and audit-trailed on every change. Above the line, the AI works for you; below, your stewards do — with the AI explaining the why.
OpenMPI speaks every healthcare standard your trust already speaks — bidirectionally, from day one. No rip-and-replace. Plug into your existing PAS, EPR, lab and NHS feeds.
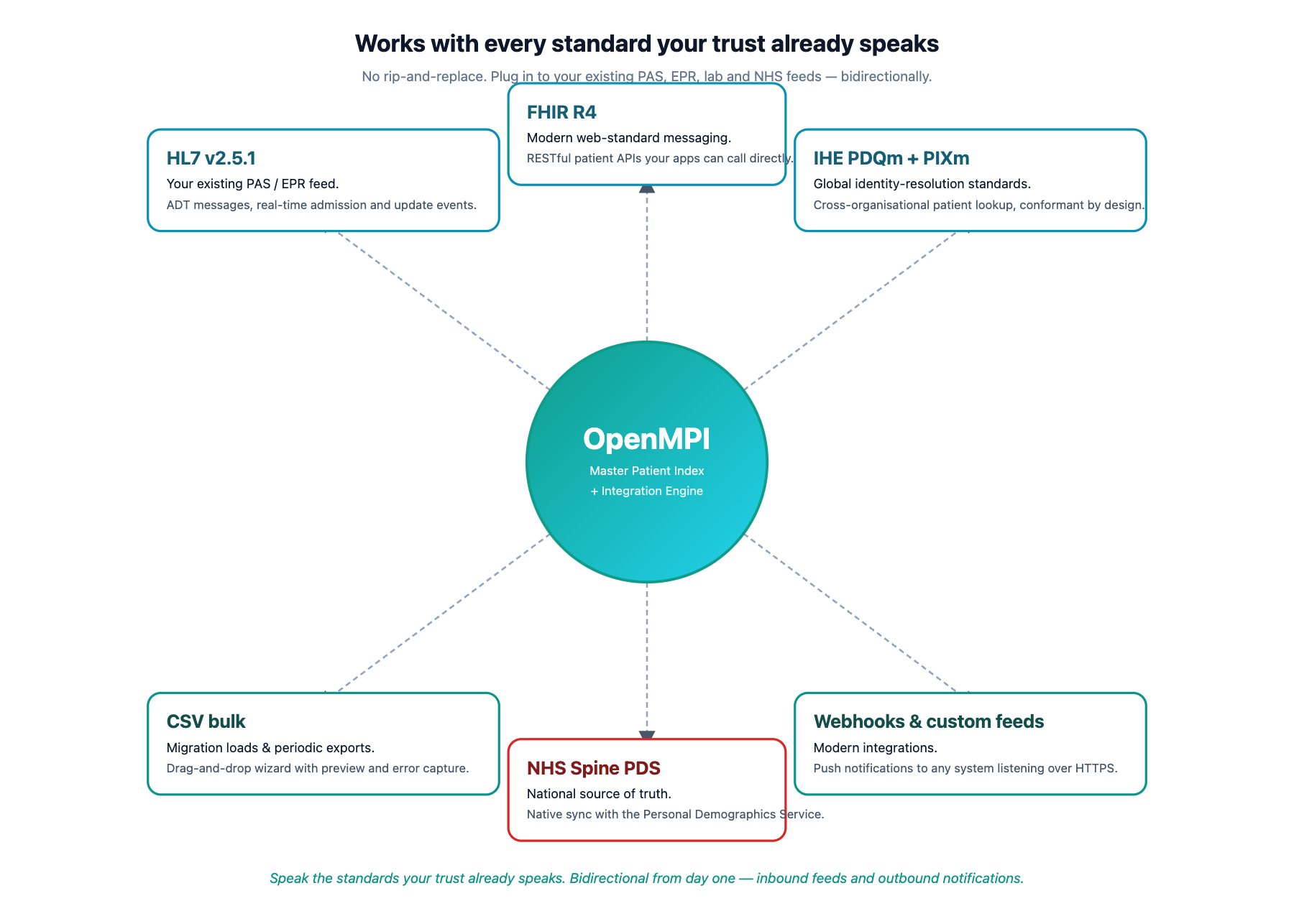
Inbound and outbound on every channel. Whether your hospital runs HL7 v2 ADT today, modern FHIR APIs, IHE-conformant identity services, or a mix — OpenMPI fits in.
Every regulatory surface that an NHS Acute MPI must satisfy — designed in, not bolted on.
Production-activation gate is explicitly closed in v0.1.x — OpenMPI is not yet authorised for live patient data. Opens v0.7+ with the NHS-ready CSCR pack and DSPT submission.
| Release | Target | Theme | Headline demo |
|---|---|---|---|
| v0.1.6a | 2026-05-06 | Doc + landing + proper login uplift | This page · 5 hand-crafted SVG architecture diagrams · 21-doc revision sweep |
| v0.1.7 | 2026-05-19 | Real PDS-FHIR + threshold lifecycle Path B | NHS PDS retrace closes Sarah O'Brien's NHS-no supersession |
| v0.2 | 2026-06-09 | Bitemporal + audit-log monthly partitioning | "What did we know about Sarah on 2026-04-15?" point-in-time view |
| v0.3 ⭐ | 2026-07-07 | First production GenAI cost gate open | Real Haiku-tier rationale (£0.0019); agent-drafted patient SMS |
| v0.4 | 2026-08-04 | Bias audit + DSPT cycle 1 | +142 cases would auto-link, CSO co-signs after KDE-valley narrative |
| v0.5 | 2026-09-08 | IHE Connectathon + HA + DSAR | HIOW Demo Tenant boots cleanly; IHE PIXm Connectathon pre-test |
8 demo personas seeded — Alice (steward), Eve (CSO), Frank (auditor), Greg (integration engineer), and four more. Sign in with any of them in seconds.